
Detailed Explanation of Iatrogenic Hypertension: Drug-Induced Blood Pressure Elevation and Prevention
Iatrogenic hypertension: Iatrogenic hypertension refers to hypertension caused by improper medication use by physicians, resulting in elevated blood pressure exceeding normal levels. It is also known as drug-induced hypertension. This type of hypertension is not common clinically. Currently, the exact mechanism of iatrogenic hypertension is not fully understood, and there is no systematic classification. It is described below based on commonly used medications.
(1) Oral contraceptives: Oral contraceptives are the most basic contraceptive method for women of childbearing age. However, some women have a potential risk of elevated blood pressure after taking oral contraceptives, with an incidence rate of less than 18%. Blood pressure gradually returns to normal after discontinuation of the medication. It is currently believed that the elevated blood pressure caused by oral contraceptives is related to the estrogen contained in the medication. Estrogen can increase renin secretion, leading to an increase in angiotensin II concentration in plasma. Angiotensin II can cause vasoconstriction, promoting sodium entry into cells; and can also increase aldosterone secretion, causing sodium and water retention, resulting in elevated blood pressure. The main treatment for this type of hypertension is to discontinue the oral contraceptive and switch to other contraceptive methods. (2) Monoamine oxidase inhibitors: These drugs include various hydrazine antidepressants, phentolamine, and furazolidone, etc. They primarily antagonize monoamine oxidase and other enzymes, hindering the inactivation of intracellular and extracellular catecholamines, i.e., preventing the inactivation of adrenaline and noradrenaline, thus increasing vasoconstriction. Clinical manifestations mainly include palpitations, systemic vasomotor activity, severe headache, facial flushing, sweating, and elevated blood pressure. About one-third of patients experience neck stiffness, nausea, and vomiting; some present with crises, such as severe exhaustion, significantly elevated blood pressure, hemiplegia, coma, or even death. Most crises do not leave significant sequelae after resolution. The key to treatment is prevention, i.e., avoiding these drugs, especially phentolamine. If a severe pressor reaction occurs, phentolamine 5-10 mg should be repeatedly injected until the severe adverse reaction disappears.
(3) Other medications: These mainly include four categories: ① Medications with glucocorticoid effects, such as glucocorticoids and licorice, whose mechanism of causing elevated blood pressure may be related to the sodium and water retention caused by glucocorticoids; ② Non-steroidal anti-inflammatory drugs (NSAIDs), such as indomethacin, which can reduce the production of prostaglandins in the body, thereby causing elevated blood pressure; ③ Hypertension caused by drugs that damage internal organs, such as phenacetin; ④ Drugs that directly cause vasoconstriction, such as ergotamine, physostigmine, and related alkaloids.
Although hypertension caused by the above-mentioned drugs is not common clinically, patients with hypertension should use these drugs with caution. When antihypertensive treatment is ineffective, the potential adverse effects of the above-mentioned drugs should also be ruled out.
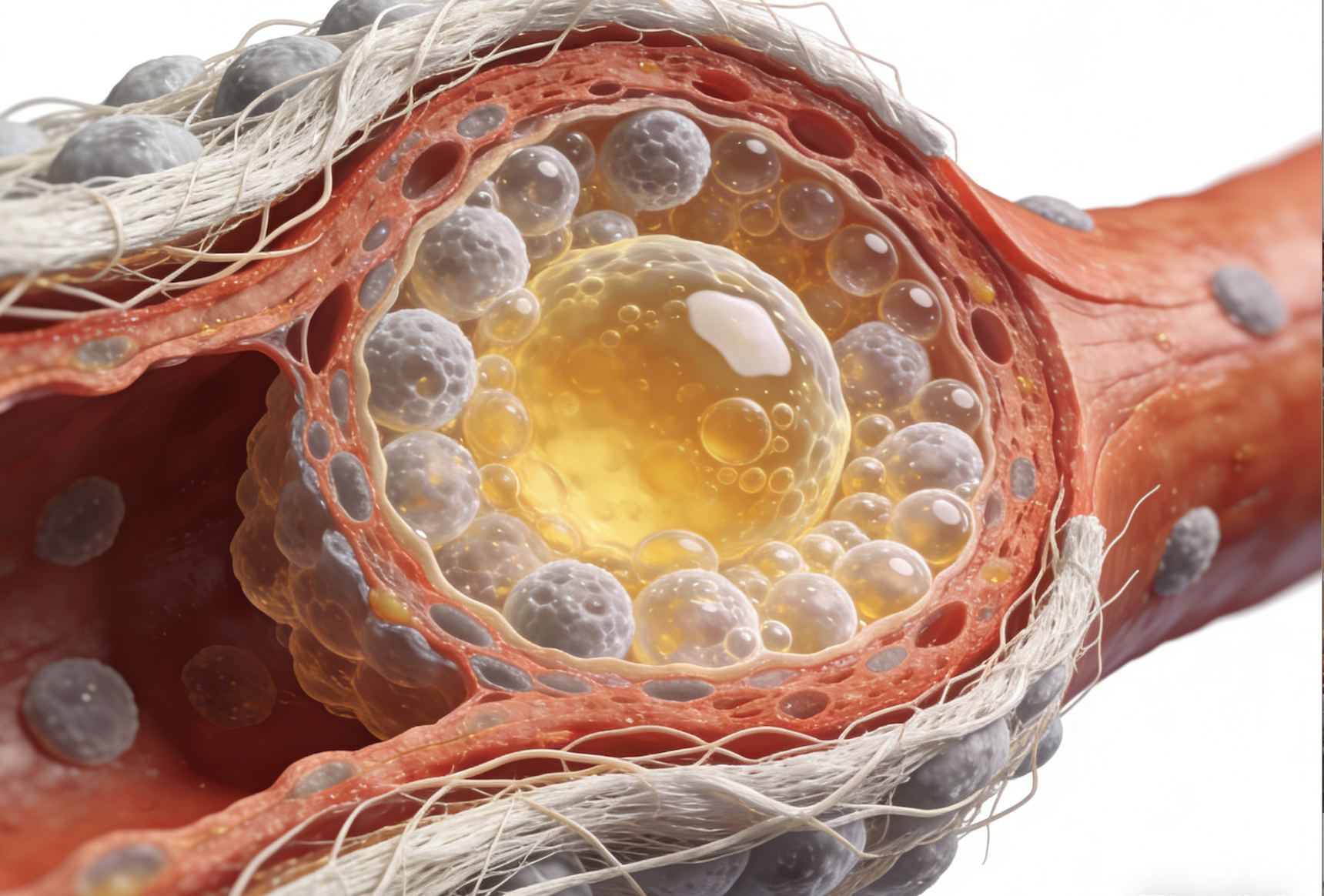
Analysis of common symptoms of hyperlipidemia: from silent onset to xanthoma manifestations
This article details the common symptoms and manifestations of hyperlipidemia (commonly known as high cholesterol), including its early, insidious nature and potential signs such as xanthomas. Understanding these symptoms helps in timely lipid testing, enabling early detection and management of lipid abnormalities.
2026-03-04
Analysis of Early Identification and Scientific Prevention Strategies for Hyperlipidemia
This article elucidates the importance of correctly understanding hyperlipidemia, revealing its hidden dangers of causing arteriosclerosis even when it is asymptomatic in its early stages. It emphasizes the necessity of lipid screening for high-risk groups and advocates for effective control of lipid levels through early intervention and scientific management.
2026-03-04
How to develop individualized lipid-lowering plans and reference standards for patients with hyperlipidemia
This article explains that the treatment of hyperlipidemia (i.e., hyperlipoproteinemia) requires an individualized lipid-lowering plan based on personal circumstances and provides specific reference values for blood lipid standards. Understanding these standards helps patients and doctors jointly set reasonable treatment goals and scientifically manage abnormal blood lipids.
2026-03-04